A 50-year-old male presents to the clinic for a rash. About one week ago, he underwent a CT scan with contrast (iohexol, brand Omnipaque) for the first time and two hours later developed an itching and burning sensation in his throat that progressed to facial swelling and diffuse redness of his skin later that evening. He was seen in the ER the next day and treated with diphenhydramine, famotidine and dexamethasone injection. Unfortunately, as the week progressed, the rash became more diffuse.
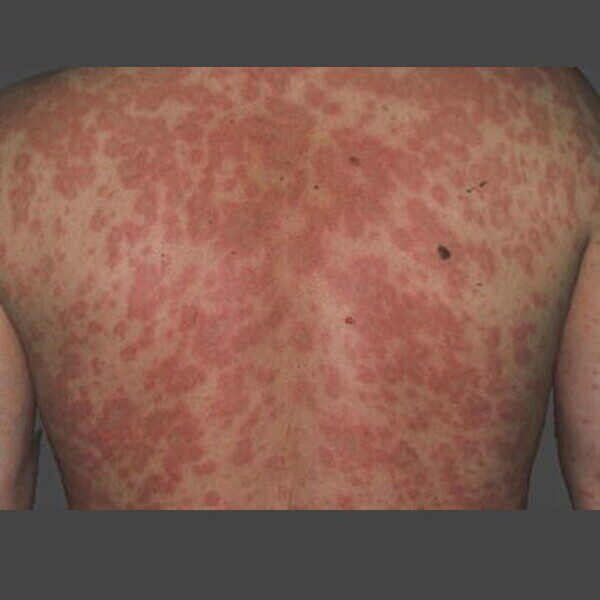
He was seen again by his primary care doctor five days later and given another dexamethasone injection and a prednisone taper. His rash is improving but he presents for additional evaluation. On exam, he has scattered erythematous macular rash occurring diffusely on his upper and lower extremities, neck, chest and back. There is no blistering of his skin. There is no peripheral eosinophilia blood work ordered by his PCP.
With reactions to contrast, it is important to first identify the implicated contrast agent, the features of the reaction, timing of onset and severity. Immediate reactions to contrast are usually within minutes to an hour of exposure and can be classified as physiologic or hypersensitivity reactions. Physiologic reactions may present as transient warmth, flushing or chills, metallic taste, nausea, vomiting, pruritus alone or hypertension. Hypersensitivity (allergic-like) reactions are relatively rare, but may include urticaria or angioedema, diffuse erythema or bronchospasm. Allergic-like reactions are not related to dose, are idiosyncratic and may not predictably occur after each contrast exposure.
Delayed hypersensitivity reactions (DHRs) to contrast occur more than one hour after contrast administration, commonly more than six hours afterwards, but can also occur up to 10 days later. Typical reactions are maculopapular exanthema or delayed onset urticaria. Studies suggest that delayed hypersensitivity reactions have a high rate of recurrence given high cross-reactivity amongst radiocontrast agents. Pre-medications are unlikely to be effective at preventing recurrence of DHRs, but they may limit the extent of reaction. Allergy testing such as skin prick, intradermal and patch testing can be utilized to help confirm the causative agent as well as identify possible alternatives, though with some variability in specificity across studies. Iobitridol has been reported to have a relatively lower risk of recurrence of DHR.